The National Commission on Local Public Health Leadership
- An introduction to public health and its top achievements
- Guidance and templates for elected officials and public health to initiate and foster partnerships
- Sample proclamation language communities can use to publicly launch a partnership commitment
- Discussion prompts for elected officials and public health leaders to lay the groundwork for coordinated action, by creating a shared vocabulary, surfacing assumptions, and clarifying roles
- Recommended action on promising areas for collaboration: data, stockpiling, and bulk purchasing
Posted on: July 15, 2026
Executive Summary
The Good Health is Good Governance toolkit by the National Commission on Local Public Health Leadership (“National Commission”) equips elected officials and local public health leaders with practical, nonpartisan ways to strengthen collaboration, enabling scientific evidence to be translated into effective policy and community action. The toolkit emphasizes a central message: durable community health and security depend on trusting relationships, foundational public health science, and shared commitment to protect the public’s health across sectors and political perspectives.
Local public health departments contribute data, scientific expertise, and operational experience; elected officials contribute democratic accountability, constituent insight, and the authority to enact and fund policy. When these strengths are aligned, communities thrive. They are better equipped to support public health and create the conditions for long-term prosperity.
The National Commission calls upon local leaders to:
- Adopt a public proclamation to formalize a shared commitment to trust-building and partnership.
- Hold regular, ongoing working sessions to strengthen collaboration and maintain alignment beyond crises.
- Clarify and document roles and decision-making authority to ensure transparency, accountability, and efficient action.
- Build and sustain a multi-sector coalition that includes key community systems (e.g., business, education, transportation, public safety, healthcare, social services, faith organizations, and residents).
- Agree on priority issues for action, including improving localized, anonymized data for decision making and strengthening preparedness for access to PPE, medicines, testing, and other essential supplies.
The toolkit focuses on partnership topics that are widely supported, foundational to community well-being, and shared responsibilities across government and sectors. It moves collaboration from abstract goodwill to concrete, repeatable practices that leaders can use to build trust and demonstrate progress to constituents.
The toolkit includes:
- A toolkit roadmap to help readers navigate this document based on their role and priorities.
- Sample proclamation language communities can use to publicly launch a partnership commitment.
- An introduction to public health that provides a shared vocabulary on what public health is, how local health departments function, and how public health systems are organized.
- The top achievements of public health, which highlight the accomplishments that contributed to adding 30 years of life expectancy and demonstrate the measurable impact of prevention, systems change, and policy.
This toolkit also offers practical strategies and guiding questions to help elected officials and public health leaders build strong collaborative relationships that support transparent, evidence-informed policymaking.
- Quick-start guide to initiating partnerships: A practical, research-informed set of tips to help elected officials and public health leaders begin working together, even without an existing relationship. It offers a spectrum of collaboration (from informal knowledge-sharing to formal agreements), principles for building trust, sample conversation scripts, and communication guidance to keep engagement constructive and nonpartisan.
- Level-setting discussion prompts: Curated questions designed to create a shared vocabulary, surface assumptions, and clarify roles between elected officials, public health leaders, and their partners before high-stakes decisions arise. These prompts are intended for one-on-one meetings, small-group discussions, retreats, or joint planning sessions and help partners identify mutual priorities, anticipate tradeoffs, and lay the groundwork for coordinated action.
- Recommended action on data: A step-by-step framework for using data to move from shared priorities to measurable progress. It guides partners to identify a priority, assess available local and regional data (and gaps), advance toward a goal with early action steps, share progress transparently with residents, and iterate through ongoing review, all supported by a sample 90-day conversation roadmap and example data sources.
- Recommended action on stockpiling and bulk purchasing: Guidance to strengthen readiness for emergencies and routine surges by clarifying how essential supplies (e.g., PPE, medicines, vaccines, testing materials) are obtained, authorized, stored, and distributed. It includes level-setting questions to map roles and decision pathways, identify supply-chain vulnerabilities, and translate lessons learned into practical next steps such as joint readiness briefings, partnerships with health systems, documented authorities, and targeted fixes to priority gaps.
These tools help local leaders build a shared understanding, establish clear decision pathways, and take visible steps on priority issues that matter to residents. The intended result is stronger governance and stronger public health through consistent communication, coordinated planning, and practical collaboration that can endure beyond political cycles.
Introduction
Public health has been integral to the United States’ success since its founding 250 years ago. It has extended life expectancy, improved community health, and made everyday life safer for millions of people. From George Washington inoculating soldiers against smallpox during the Revolutionary War to contemporary efforts to ensure safer workplaces or reduce chronic disease, public health remains the engine that keeps the country moving forward.
These great public health achievements result from collaboration across sectors and levels of government. The Bipartisan Policy Center’s 2021 report, Public Health Forward: Modernizing the U.S. Public Health System,1 outlines a clear vision for a 21st-century public health system and underscores a central truth: strong public health depends on technical capacity, trusting partnerships, and shared commitment across political perspectives and sectors.
Central to this shared responsibility is the collaborative relationship between local health officials and policymakers. Local health departments and public health professionals bring scientific expertise, data, and on-the-ground experience. Elected officials bring democratic accountability, community insight, and the authority to enact and fund policy. Each role is essential; together, they translate knowledge into action and achieve outcomes that neither party could achieve alone. When these strengths are aligned, communities are better prepared to prevent harm, respond to crises, and create the conditions for long-term prosperity.
As the United States approaches its 250th birthday, the country has a chance to celebrate its progress and invest in a future that protects health, saves lives, and ensures liberty and justice for all.
This report draws on insights and experiences from leaders across the country and offers a path forward to ensure that the health and well-being of all communities remain a defining strength of the nation for generations to come.
The recommendations in this report come from the National Commission on Local Public Health Leadership (“National Commission”), which was established in July 2025 to develop a unified, actionable vision for public health that prioritizes the health and well-being of every American. It aims to address fundamental questions about the role of science in policymaking and foster alignment between public health and policy. The National Commission includes members with expertise in public health, policy, medicine, business, and lawmaking. More information on Commission members can be found in Appendix A.
The de Beaumont Foundation, whose mission is to advance policy, build partnerships, and strengthen public health to create communities where everyone can achieve their best possible health, created this report to guide the future of public health practice.
Strengthening relationships between public health professionals and elected officials is essential to translating scientific evidence into policies that protect and promote community well-being. Collaborative relationships are a cornerstone of improvements in a community’s health.
The National Commission designed this toolkit to make relationship-building more concrete by providing “starter” topics for discussion. Its goal is to advance the vision set forth in Public Health Forward by equipping elected officials and local public health leaders with shared language and actionable strategies to build and sustain strong connections.
It supports public health practitioners, elected officials, and community partners in building trust, aligning around evidence, and advancing policies that reflect both scientific knowledge and constituent priorities. By working across perspectives and focusing on common purpose, leaders can improve decision-making and build systems that endure beyond political cycles.
The National Commission calls upon elected and local public health officials to commit to the following actions, at minimum, to pursue optimal health for their community.
- Formally adopt a proclamation to publicly memorialize the commitment to build trust and partnership between elected officials and public health officials.
- Publicly agree to regular and ongoing working sessions to improve the strength and security of the community by rebuilding trust in and commitment to public health.
- Agree to and memorialize decision-making authority and roles in ways that are consistent, transparent, accountable, respectful, and in pursuit of optimal community health.
- Agree to build and sustain a multi-sector coalition (partnerships) for public health to include business, education, transportation, agriculture, public safety, healthcare, social services, faith institutions, and residents with lived experience.
- Agree on priority issues for action, including but not limited to improving localized, anonymized data to guide decision-making; plans to acquire PPE, medicines, and testing in the event of emergencies; and other issues as identified by local priorities and community interests.
The priority actions highlighted in this toolkit — mutually identifying local priorities, strengthening localized data, and ensuring reliable access to PPE and other emergency supplies — were intentionally selected.
These topics are:
- Widely agreed upon. They are practical, nonpartisan issues that both elected officials and public health leaders can readily support.
- Fundamental to community health. Each directly affects a community’s ability to prevent harm, respond to crises, and promote long-term well-being.
- Shared responsibilities. None of these issues can be effectively addressed by one sector alone. They require coordination, clarity of roles, and ongoing communication between public health and elected leadership.
- Concrete and actionable. They move partnership from abstract goodwill to tangible collaboration with visible decisions, investments, and accountability.
By focusing on these areas, elected and public health officials build relationships around real work that matters to constituents. These topics create structured opportunities to clarify expectations, strengthen trust, and demonstrate a mutual commitment to protecting and improving community health.
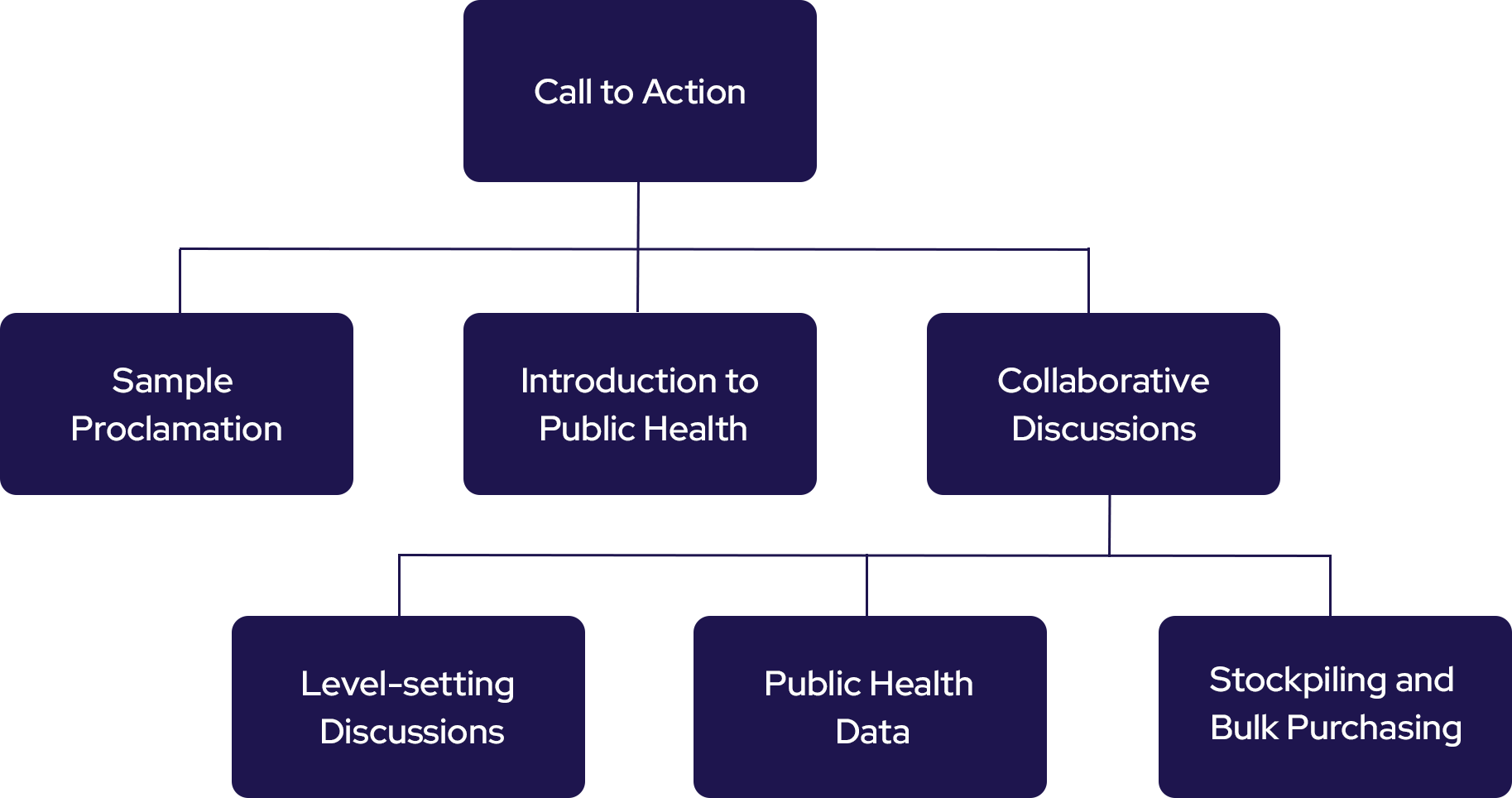
This roadmap provides a visual overview of how this toolkit is organized and how the different sections build upon one another. Public health and policymaking are both complex, relationship-driven fields, and readers may engage with this toolkit from different starting points depending on their role, priorities, or community needs.
The roadmap is intended to help elected officials, public health leaders, and partners quickly understand the structure of the toolkit, navigate to the most relevant sections, and see how foundational concepts — such as public health orientation, collaborative discussions, data use, and preparedness planning — connect to broader action and decision-making. By illustrating the flow of the toolkit, this section helps create a shared understanding of the journey from conversation to coordinated community action.
The de Beaumont Foundation and the Kasich Company would like to recognize and thank the members of the National Commission on Local Public Health Leadership for their guidance and support, as well as Dr. Anand Parekh for serving as Special Advisor to the Commission.
Sample Proclamation
Introduction
The National Commission on Local Public Health Leadership encourages communities ready to strengthen trust between elected officials and public health leaders to formalize that commitment through an official proclamation and publicly promote the effort.
An official proclamation recognizes an issue, establishes a clear statement of intent, and signals that local leaders are aligned in their commitment to community health and are willing to be publicly accountable for it. By placing the effort on the public record, a proclamation elevates the importance of collaboration in effective governance and communicates that improving health outcomes is a shared civic priority.
In this way, a proclamation becomes an early and visible step toward sustained partnership, demonstrating that local leaders are committed to working together to strengthen trust and advance the health of the community.
Sample proclamation language can be customized for each community.
A SHARED COMMITMENT TO PUBLIC HEALTH ACTION — PROCLAMATION TEMPLATE
WHEREAS, public health is a united effort to protect health and save lives; and
WHEREAS, during the 20th century, life expectancy among U.S. residents increased by nearly 30 years — from 47.3 years in 1900 to 76.8 years in 2000 — and approximately 25 years of this gain are attributable to advances in public health; and
WHEREAS, strong public health systems contribute to thriving communities, economic stability, emergency preparedness, and informed decision-making; and
WHEREAS, elected leaders and public health leaders share a responsibility to make decisions transparently, communicate clearly, and consider the best available evidence alongside community needs and perspectives; and
WHEREAS, a shared understanding of responsibility, authority, and the role of science that respects diverse perspectives strengthens collaboration between public health leaders and elected leaders responsible for policies that impact the community; and
WHEREAS, a sustained commitment to transparent communication and constructive engagement is necessary to build an enduring vision to guide the evolving landscape of public health policy in our community;
NOW, THEREFORE, BE IT PROCLAIMED that [COMMUNITY NAME] shall convene regular, ongoing working sessions among local elected leadership and public health leadership to rebuild trust in — and commitment to — public health; and
BE IT FURTHER PROCLAIMED that [COMMUNITY NAME] shall memorialize clear roles, decision-making authority, and shared expectations for collective public health action that are consistent, transparent, accountable, and aligned with a strong, thriving community; and
BE IT FURTHER PROCLAIMED that [COMMUNITY NAME] shall build and sustain a multi-sector public health team that includes and engages partners across key sectors; and
BE IT FURTHER PROCLAIMED that [COMMUNITY NAME] shall identify and advance priority issues for local public health action, which may include preparedness and the strengthening and localization of public health data.
PASSED AND APPROVED this ____ day of ________, 2026.
Introduction to Public Health
Policymakers make decisions every day that shape the conditions in which people live, work, learn, and age. Public health professionals work every day to protect and improve community health. While their roles are different, their goals often overlap. Strong communities, stable systems, and effective responses to crises depend on both groups understanding how their work connects.
The National Commission on Local Public Health Leadership provides this Public Health Primer to help elected officials gain a broad understanding of public health and to help public health officials explain their role in promoting and protecting community health.
This primer provides a clear, plain-language overview of what public health is, how it functions, and why it matters. It is not meant to make policymakers into public health experts, nor to restate what public health professionals already know. Instead, it offers a shared vocabulary and baseline understanding that can support productive conversations and practical collaboration.
Public health is a field dedicated to protecting and improving the health and safety of all people and communities. Public health looks at the bigger picture: What makes people more likely to get sick or injured? What conditions help them live longer, healthier lives?
The de Beaumont Foundation studied and identified five key public health concepts to build understanding of public health, its role in communities, and its value and importance:
- Public health works at the community level, while healthcare works at the individual level.
- Public health focuses on preventing people from getting sick or hurt.
- Public health workers serve their local communities.
- Public health workers have a variety of professional roles, and many work behind the scenes.
- Public health benefits everyone.
Public health professionals across the country work to promote well-being in their communities. They have diverse roles and titles, such as epidemiologist, community health worker, data analyst, inspector, planner, and evaluator. They work on a variety of topics, including access to clean water, sanitation, emergency-response services, maternal health, mental health, food safety, lead poisoning prevention, and infectious disease management. Together, these public health workers have implemented countless initiatives that have saved lives and significantly improved the duration and quality of life in the United States.2

Image adapted with permission from the National Association of County and City Health Officials.
Public health work happens at the local, state, and federal levels, but most people experience it closest to home through their local health department, where policies, programs, and services directly touch their daily lives.
In short, local health departments work both behind the scenes and on the front lines to keep communities safe, informed, and healthy.
There are approximately 2,800 local health departments across the United States. In addition, there are 59 state and territorial health agencies (including all 50 states, D.C., and U.S. territories) and numerous Tribal health departments.
Some public health departments serve a single city or county, while others serve regional areas. They vary significantly in terms of staffing and services offered.
Local and state health departments are structured based on governance models:
Centralized
Operated and staffed by the state health department
Decentralized
Operated independently and governed by local authorities
Shared or Mixed
Joint oversight by local and state governments
Health department reporting depends on governance:
- Local health departments report to boards of health, county commissioners, or city councils.
- State-run units report to state health agencies and ultimately to governors or state leaders.
- Tribal health departments report to sovereign Tribal councils.
Public health practice and research are supported by a multi-sector network of partners, including:
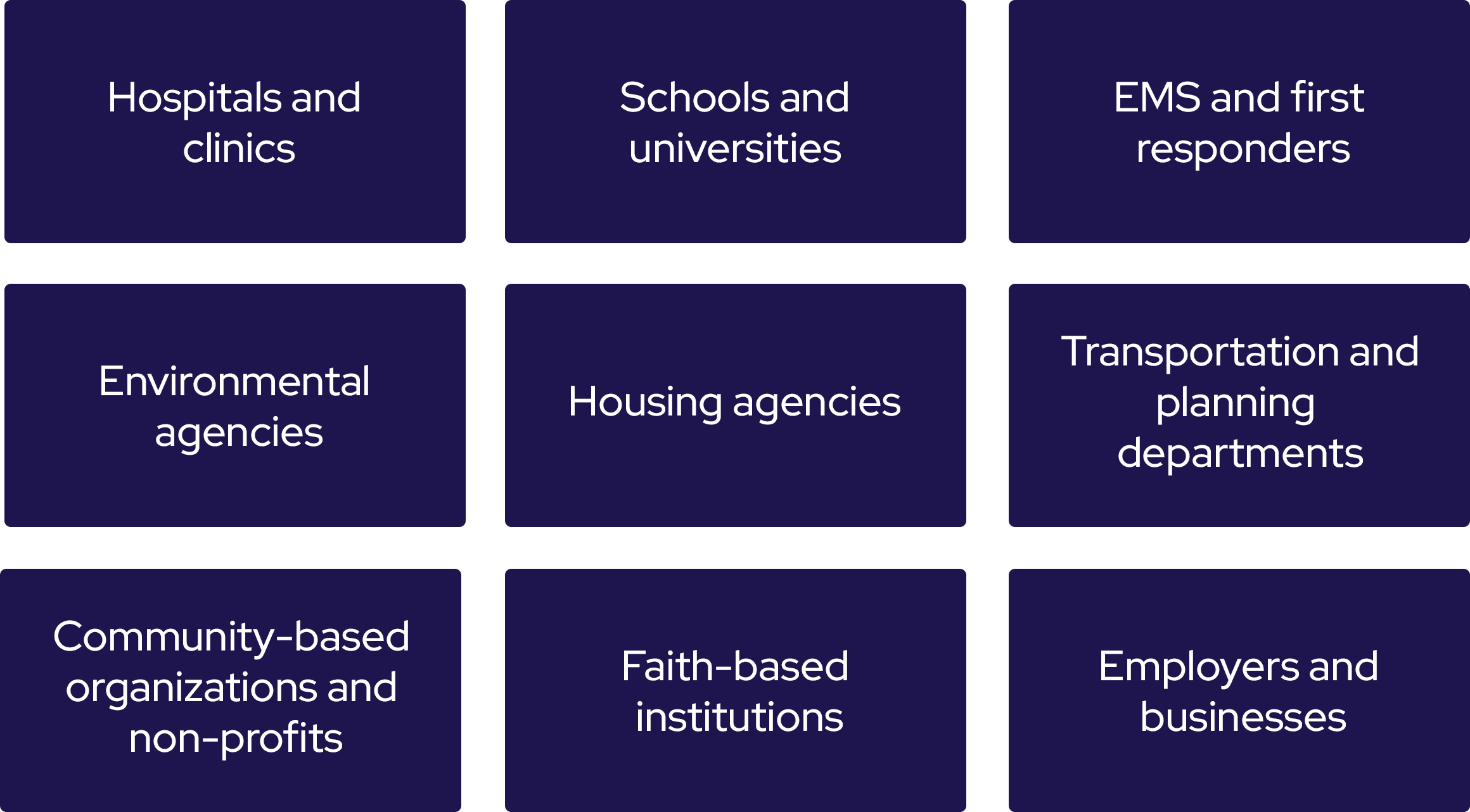
These collaborators form a comprehensive public health system, addressing community health needs and promoting community resilience.
As a result of engaging these multi-sector partners, local public health leadership can be defined as the interdependent relationship among public health practitioners, elected officials, and cross-sector leaders, and the entities they represent, that are responsible for guiding, managing, and advocating for public health efforts within a specific community, city, or region.
Collectively, these leaders play a critical role in protecting and improving the health of communities through decision-making, strategic planning, and collaboration with stakeholders to promote optimal health for all and respond effectively to local public health needs.
Top Public Health Achievements
Public health has helped people live longer, healthier lives. Many of the advances described below were made possible through collaboration among local health departments, policymakers, community leaders, and federal partners. While the topics in this list are not policy recommendations of this toolkit, they demonstrate that public health is a practical field with a proven track record of delivering measurable results. They ground the toolkit in evidence and possibility, signaling that today’s complex challenges can also be addressed through partnership and sustained commitment.
Through the combined efforts of elected officials and public health leaders to enact codes and establish health standards, significant improvements in public health outcomes have been achieved. The United States saw its first local health boards in the late 1700s, and by 1900, they were commonplace.1 During the 20th century, life expectancy in the United States increased by more than 30 years, with approximately 25 of those years attributed to advances in public health. Rather than resulting from medical treatment alone, these gains were largely driven by prevention, systems change, and policy interventions that reduced exposure to risk and improved living conditions for entire populations.2,3
The impact of these efforts can be seen in:
Control of Infectious Diseases
Improved access to vaccines dramatically reduced deaths from infectious diseases such as tuberculosis, typhoid, and cholera. Public health surveillance, outbreak response systems, and the development of antibiotics further reduced deaths from infectious threats.
Water, Sanitation, and Hygiene
The U.S. began focusing on water, sanitation, and hygiene in the 1700s and 1800s. Environmental sanitation through the creation of sewers, refuse removal, and proper ventilation, for example, helped prevent typhoid, cholera, and other infectious diseases of the time. These elements of environmental sanitation remain pillars of effective disease prevention.
Motor-Vehicle Safety
In the early 1900s, motor-vehicle crashes were a growing cause of death. Over time, coordinated efforts — including safer vehicle design, traffic laws, driver education, licensing requirements, and roadway engineering — significantly reduced traffic-related fatalities and injuries.
Safer Workplaces
At the start of the century, workplace injuries and deaths were common, particularly in mining, manufacturing, and construction. Safety regulations, labor protections, engineering controls, and monitoring systems led to substantial reductions in occupational injuries and fatalities.
Decline in Deaths from Coronary Heart Disease and Stroke
Beginning in the mid-20th century, deaths from heart disease and stroke declined significantly. This shift was driven by increased awareness of risk factors (such as high blood pressure and cholesterol), improvements in emergency response and treatment, and population-level changes in diet, physical activity, and smoking rates.
Safer and Healthier Foods
Food safety systems were strengthened through inspections, pasteurization, refrigeration, and improved food-handling practices. These efforts reduced food-borne illnesses and nutritional deficiencies and improved overall population health.
Recognition of Tobacco Use as a Health Hazard
The identification of smoking as a cause of lung cancer and other chronic diseases marked a turning point in public health. Public education campaigns, warning labels, policy restrictions, and community interventions helped significantly reduce smoking prevalence and related deaths.
Overall Impact
These achievements show how prevention and population-wide interventions can effectively complement individual medical care. Improvements in sanitation, safety standards, surveillance systems, education, and policy infrastructure transformed everyday environments, making homes, workplaces, roads, and food systems safer.
Collectively, these efforts have reshaped the health landscape of the United States and contributed substantially to longer, healthier lives.
Initiating Partnerships: A Quick-Start Guide
Despite a polarized national political climate, local leaders consistently find ways to work together and rise above the noise. They are accountable to the same people and care about the same place: their community. For both elected officials and public health leaders, creating meaningful, positive change requires working in close partnership, grounded in strategy, coordination, and collaboration.2
Initiating collaborations can feel vague in practice. This brief guide, drawn from political science2 and public health research, provides practical tips for calling meetings and initiating conversations, even when the local elected and public health officials have no pre-existing relationship.

Figure based on the text from the book Collaborate Now!2
Partnerships can vary based on the specific needs, available resources, and goals of each partner, and can change over time. Many existing collaborative relationships are formal, held through contracts or other formal agreements with understood roles and deliverables. While they are beneficial, formal collaborations are not required for collective action in a community.
Equally important are informal collaborations. The relationship-building conversations recommended by the National Commission on Local Public Health Leadership are well-suited for informal collaboration. These collaborations can be for sharing expertise to inform decisions, addressing specific questions or topics, or brainstorming and building ideas. While informal collaborations are not tied to contracts or deliverables, they are critical, low-cost ways to build trust and rapport between partners.

When leaders engage in creating and building partnerships, they should keep these research-backed principles in mind:

- Shared purpose: Emphasize that elected officials and public health leaders are on the same team, serving the same community.
- Local expertise: Leverage local expertise and locally rooted knowledge to discuss what is feasible for the community.2
- Practicality: Focus on what’s realistic, relevant, and useful in each community’s specific context.
- Curiosity: Approach conversations with warmth and see them as opportunities to learn. Maintain a “culture of learning,” not a “culture of knowledge.”2
- Humility and respect: Value the expertise and perspectives of the other person and use meetings efficiently to honor their time.
- Presence: Showing up matters, and repeated interactions build trust. Have in-person conversations, attend community events, and follow up after meetings.
Given these key principles, public health leaders wishing to engage local elected officials can use the prompting language below to initiate conversations.
The goal is not to test knowledge or drive immediate decisions, but to create space for curiosity, clarity, and shared understanding.
Public Health Initiating a Conversation with a Policymaker
- “I’d welcome a 30-minute conversation to better understand your priorities related to community health and share what we’re seeing locally. My goal is to identify where our work can best support yours.”
- “I’d appreciate the opportunity to connect over coffee and learn what’s top of mind for you. We can also share relevant data and community insights that may be useful as you consider next steps.”
- “I’m hoping to meet to discuss [issue]. I’d like to (1) hear your priorities and constraints, (2) share key data and community perspectives, and (3) explore practical opportunities to align efforts.”
Why this works:
- Signals appreciation for the policymaker’s role and priorities
- Positions public health as a supportive asset
- Sets clear goals for the conversation
Policymaker Initiating a Conversation with Public Health
- “I’m interested in strengthening coordination between our offices and would welcome a conversation next week about shared priorities and opportunities to collaborate.”
- “I’d like to connect to learn more about what you’re seeing in the community, particularly around [issue]. Your perspective would be valuable as we consider next steps. Are you available for a 45-minute call next week?”
- “As we look at [issue], I’d appreciate a conversation to better understand the public health implications and any data that should inform our approach.”
Why this works:
- Invites shared expertise in a focused way
- Shows that public health input is valued early
- Sets foundation for ongoing collaboration
Framing the Value of Connecting
- “We can share timely data and community insight, and learning your priorities helps us focus where we can be most useful.”
- “We’re hearing consistent themes from residents on [issue], and connecting those perspectives with your leadership could strengthen solutions.”
- “You bring a policy and governance lens, and we bring population data and community relationships — together, that can lead to more actionable solutions.”
Why this works:
- Emphasizes mutual benefit and shared responsibility
- Highlights respective strengths of each party
- Lets the other party know their time would be well spent
Pitfalls to Avoid When Initiating Conversations
- “I need you to do X.”
- “We need you to support this initiative.”
- “I’d love to connect about health and collaboration.”
Why these won’t work:
- Leading with a demand leaves no room for discussion
- The outreach is transactional
- The invitation is vague, and there is no clear signal of the goals of the conversation or how the person’s time will be used effectively
The following tips, based on the “Communicating About Public Health with Policymakers” toolkit, 3 share three principles that resonate well when engaging policymakers in public health. These approaches increase trust-building and motivate stakeholders to champion public health by focusing on what is possible.
- Show aspirational impact: Position public health as a force that strengthens both local well-being and economic vitality, rather than something that inherently requires a tough tradeoff.
- Emphasize a local, listening-based approach: Show that public health recommendations are based on listening to communities about their needs, not on an ideological agenda.
- Highlight how community health leads to individual control: Demonstrate that community health and individual control are complementary. When communities are healthier, people can make healthier choices for themselves and their families.
The toolkit includes additional resources such as messaging do’s and don’ts, exercises to implement these tips, and sample language, drawn from focus groups and in-depth research with policymakers.
A 2025 poll from the de Beaumont Foundation and the Harvard Opinion Research Program (HORP) challenges common media narratives that the U.S. is hopelessly divided, revealing bipartisan support for key public health priorities.4 In particular, broad swaths of the public across political parties share many top priority issues for state public health agencies to address in the next four years, including:
- Preventing chronic diseases (85% of Republicans, 86% of Democrats)
- Protecting against new viruses that could become pandemics (69% of Republicans, 92% of Democrats), and
- Addressing opioid and other substance addiction (76% of Republicans, 83% of Democrats).
There are also commonalities that might not be expected within specific public health policy areas, such as support across parties of routine childhood vaccination requirements for children to attend school: 79% of Americans — including 90% of Democrats, 68% of Republicans, and 66% of Make America Great Again (MAGA) supporters — support requiring routine childhood vaccines.
Recommended Action: Level-Setting Discussions
This section of the toolkit offers introductory and level-setting questions designed to spark meaningful dialogue between elected officials and public health leaders. The goal is not to test knowledge or drive immediate decisions, but to create space for curiosity, clarity, and shared understanding.
Public health touches many areas: emergency preparedness, chronic disease prevention, data and measurement, workforce capacity, funding structures, community partnerships, and more. Yet partners may come to these topics with different experiences, assumptions, and priorities. These questions are designed to surface those perspectives in a constructive way.
The National Commission recommends that public health officials meet with local elected officials and use these prompts in one-on-one meetings, small-group discussions, retreats, or joint planning sessions. Some questions focus on clarifying roles and responsibilities. Others explore values, tradeoffs, and opportunities for alignment. All are intended to help participants:
- Build a shared vocabulary
- Identify areas of mutual interest or concern
- Surface potential misunderstandings early
- Lay the groundwork for collaborative action
There are no right or wrong answers. The value lies in the dialogue itself. By discussing these questions openly and thoughtfully, partners can move from assumptions to understanding, and from understanding to coordinated, forward-looking leadership in service of community health.
These questions are meant to seed public health-focused conversations and uncover elected officials’ priorities.
“What are the top three health risks and top three health opportunities in our community right now? How do they connect to community goals (jobs, schools, public safety, economic stability)?”
Purpose: forces prioritization, ties public health to “strength and security,” and creates a shared agenda beyond emergencies.
“In your professional opinion, what public health accomplishments have most improved community prosperity and security over the last 25 years and over the last century? How can we translate those achievements into clear local ‘wins’ we can communicate?”
Purpose: surfaces concrete success stories, anchors public health to prosperity outcomes, and creates a shared menu of proof points for branding, messaging, and accountability.
“In a hypothetical emergency or fast-moving situation, what decisions are clearly yours by law, what decisions are clearly mine, and where do we need to make them together? How do we clearly communicate these decisions to staff and the public?”
Purpose: clarify who declares what, who issues guidance vs. orders, who controls resources, who speaks publicly, and how disagreements get resolved.
“If an emergency hit tomorrow, what capabilities do we have locally for the first 72 hours (e.g., PPE, medicines, testing, staffing, surge sites) and what are the gaps? What’s our plan to bridge to state and federal support (including the strategic national stockpile)?”
Purpose: turns “preparedness” into a concrete checklist; prompts discussion of local stockpile, bulk purchasing, supply chain transparency, and who authorizes spending.
“How will we communicate together so the public hears one clear message that is aspirational, non-ideological, and respectful of individual choice, while still explaining the ‘why,’ the limits of evidence, and what success looks like?”
Purpose: assigns spokesperson roles, pre-bakes message principles, creates a feedback loop for trust, and includes a plan to report out joint successes.
“Who else needs to be at the table to build a durable and prosperous public health coalition for our community? What specific roles should partners across healthcare, business, education, public safety, social services, and faith institutions play?”
Purpose: identifies missing voices, clarifies partner value, and converts “coalition” into named seats, responsibilities, and a plan for sustained engagement.
Recommended Action: Improving Public Health Data
In addition to building local familiarity with and increasing the use of data to prioritize community health issues, the National Commission on Local Public Health Leadership also calls for more efficient data collection and use by data actors, including healthcare systems, public health organizations, and their partners.
Sound decision-making to improve the community’s health in both governance and public health depends on reliable, relevant data. When used effectively, data help illuminate community needs, identify disparities, guide resource allocation, strengthen accountability, and measure progress over time.
Historically, public health data systems were built around reporting to the federal level:

This model does not work well in a rapidly changing environment where communities need timely insights to respond to chronic disease, behavioral health crises, maternal health challenges, environmental threats, and emergency events.
Therefore, improving data usability for communities needs a different approach:2
- Data should flow back to local leaders in usable forms
- Population-level information should be easier to access
- Systems should reduce duplication and repetitive reporting
- Healthcare, public health, and community systems should work together
- Communities should use shared information to guide local action
These six principles are intended to help local elected officials, public health leaders, and community partners build stronger, more practical approaches to using and sharing public health data. Together, they support faster decision-making, improved coordination across sectors, more efficient use of resources, and greater public trust.
They are included in this toolkit to help local leaders move toward data practices that are actionable, accessible, and grounded in real community needs regardless of local size, geography, or capacity.
1. Collect Data Once, Use It Often
Communities should reduce duplicative data collection whenever possible.
Information that is already collected by hospitals, healthcare systems, public agencies, or community organizations should be structured so it can support multiple purposes:
- Clinical care
- Population health
- Emergency response
- Policy decisions
- Community planning
The more communities rely on disconnected systems and one-off reporting requests, the harder it becomes to act quickly and efficiently.
2. Empower Communities Through Accessible Data
Local leaders cannot respond to problems they cannot see. Communities need timely access to:
- De-identified population health information
- Local trends and indicators
- Data that is understandable and actionable
- Information that reflects local conditions
Public health data should not remain locked inside isolated systems, expensive contracts, or highly technical environments inaccessible to local decision-makers.
3. Build Trust Through Transparency and Accountability
Communities increasingly expect visible progress, transparency, and responsiveness from institutions.
Data helps communities:
- Demonstrate progress
- Identify gaps
- Allocate resources more effectively
- Show accountability
- Build public trust
Trustworthy institutions are transparent about both successes and challenges.
4. Not All Data Needs the Same Level of Access
When there is a call for more data collection or sharing, many questions arise around privacy, security, and legality. Some information requires significant protections, while other data can safely be shared publicly in de-identified forms.
Data holders and sharers should distinguish between:
- Individual protected information
- Sensitive operational data
- De-identified population-level trends
- Publicly shareable indicators
This distinction can help reduce unnecessary barriers to collaboration while still protecting privacy.
5. Smaller Communities Can Still Participate
Rural and lower-resource communities may not have dedicated analysts or advanced technology systems.
Communities can still make substantial progress by:
- Using publicly available datasets
- Partnering regionally
- Working with universities or intermediaries
- Starting with a few priority indicators
- Building simple dashboards or shared reports
The goal is progress, not perfection.
6. Technology Alone Will Not Solve the Problem
Interoperability and modern tools matter, but relationships remain essential.
Communities improve outcomes when:
- Partners trust one another
- Leaders align around shared goals
- Data is connected to action
- Community voices help interpret findings
Data systems are ultimately tools for collaboration and decision-making.
The tables below include lists of commonly used data sources to address public health issues. While these lists are not exhaustive, they provide starting points for examining what population-level data is readily available.
Federal
- US Census and American Community Survey
- CDC WONDER and PLACES
- National Center for Health Statistics
- Behavioral Risk Factor Surveillance System
- Pregnancy Risk Assessment Monitoring System
Nationwide, with location-specific data
- CityHealth Dashboard
- Big Cities Health Coalition
- Congressional District Health Dashboard
- America’s Health Rankings
- Kaiser Family Foundation
- popHIVE
State and local
- State and local health departments
- Community Health Needs Assessments
- Universities
- Health Information Exchanges
- School systems
- Housing systems
*These organizations or services operate nationwide and provide location-specific data, and are separate from federally provided (e.g., CDC, HHS) data.
| Health Measures | State or Local Data Sources | National or Federal Data Sources |
|---|---|---|
| High school graduation rates |
|
|
| Full-time employment rates |
|
|
| Water quality |
|
|
| Chronic disease |
|
|
| Injuries and injury prevention |
|
|
Recommended Action: Stockpiling and Bulk Purchasing Partnerships
Public health depends on reliable access to essential supplies to maintain routine services and, most critically, to respond to emergencies. These can include personal protective equipment (PPE), vaccines, antibiotics, antiviral medications, testing materials, and other critical items. Two common strategies help ensure that these supplies are available when needed: stockpiling and bulk purchasing.
For local elected officials and local public health leaders, familiarity with these systems is essential. Leaders should understand where their community’s supplies come from, how requests are made, what authorizations are required to access state or federal resources, and what gaps may exist. Even outside of emergencies, routine immunization efforts, disease outbreaks, and seasonal surges depend on clear procurement processes and strong intergovernmental relationships.
More details, including existing bulk purchasing and stockpiling mechanisms across states, are included in Appendix B.
Stockpiling refers to maintaining reserves of key supplies in advance of emergencies. These reserves may be managed at the federal, state, or local level. When supply chains are disrupted or demand surges, communities can access materials quickly through stockpiles rather than competing for limited resources.
Bulk purchasing involves buying supplies in large quantities, often through state or federal contracts, regional purchasing cooperatives, or multi-jurisdiction agreements, to secure better pricing and more stable access. This approach can stretch limited public dollars and reduce the risk of shortages during both routine operations and emergencies.
The National Commission on Local Public Health Leadership identified stockpiling and purchasing as a critical and concrete area of alignment for elected officials and local public health workers. Local officials should discuss each of these questions to build a shared understanding of stockpiles, how to access them, and how to enhance their ability to respond to the next emergency.
The National Commission provides some discussion questions to foster shared understanding, clarify expectations, and strengthen collaboration before urgent decisions must be made. These questions can inform ongoing meetings among elected officials, public health workers, and their partners and naturally lead to tangible next steps.
1. What essential supplies are most critical based on our community’s risks and past experiences?
Potential barriers to access
Where do we see potential vulnerabilities in the supply chain we can access?
Consider supplies needed across sectors, including:
- Personal Protective Equipment (PPE)
- Medications and vaccines
- Testing materials
- Sanitation and cleaning supplies
- Equipment for first responders
- Supplies to support community members
2. How does our community currently access essential supplies during normal operations — and how does that process change during an emergency?
This includes:
- Purchasing systems
- Emergency procurement
- Vendor relationships
- Distribution during emergencies or times of increased demand
3. What local, state, or federal stockpiles are available to us, and what steps are required to request or receive those resources?
This includes:
- Existing resources
- Eligibility requirements for specific partnerships or access points
- How to submit requests for supplies
- Timelines for receiving supplies
- Potential barriers to access
4. Where do we see potential vulnerabilities in the supply chain we can access?
This can include:
- Dependence on a single vendor
- Local storage capacities
- Transportation issues
- Staffing issues
- Competition for supplies during emergencies
5. What roles and authorities do elected officials and public health leaders each hold during emergencies?
Clarify:
- Who authorizes purchases
- How emergencies are declared, and by whom
- Mutual aid agreements
- Communication responsibilities
6. What lessons did we learn from recent public health emergencies about access to supplies, and how have those lessons informed current policy or practice?
Consider:
- What went well
- What created confusion and delays
- Which partnerships were valuable
- What operational or policy changes have been made since then
7. How can we communicate clearly with residents about supply availability and preparedness efforts in ways that build confidence rather than alarm?
Discuss:
- Potential trusted messengers
- How to have clear and consistent communication
- Managing false narratives
- Maintaining transparency during challenges
- Public expectations during emergencies
The following action steps can help communities operationalize the ideas discussed in this section by translating conversations into concrete practices, formal agreements, and ongoing collaboration. These actions are intended to improve readiness before emergencies occur, reduce confusion during high-pressure situations, and create lasting systems that support faster, more coordinated responses over time.
Conduct a Joint Supply Readiness Briefing
Schedule a standing briefing with local public health leadership, key elected officials, healthcare leaders, and other partners to review how essential supplies are obtained, stored, and distributed for essential health workers (healthcare, public health, environmental services/sanitation, first responders, etc.). This should include an overview of current stockpiles, purchasing contracts, approval authorities, and the process for accessing state or federal resources. The goal is to ensure shared understanding before an emergency occurs.
Engage with Hospitals and Healthcare Systems
Healthcare systems often have mechanisms for bulk purchasing supplies. Elected officials and public health leaders should partner with these systems to gain familiarity with how critical supplies are purchased, stored, or accessed, and seek partnerships with pre-existing mechanisms to obtain such supplies.
Clarify Partners, Roles, and Decision Pathways in Writing
Document who has authority to declare an emergency, approve emergency expenditures, request access to state or federal stockpiles, and communicate with the public. Confirm that both elected officials and public health leaders understand these roles. Clear documentation reduces confusion and speeds response when time is limited.
Identify and Address One Supply Vulnerability
Using recent experience or discussion, identify one realistic gap in your community’s supply readiness, such as limited local PPE reserves, unclear procurement timelines, or reliance on a single vendor. Develop a practical plan to address that vulnerability, whether through updated contracts, participation in a purchasing cooperative, or modest local stockpiling. Taking one concrete step builds momentum and strengthens preparedness over time.
Conclusion
At its core, the National Commission on Local Public Health Leadership’s call to action is to move from parallel work to purposeful partnership.
Healthy communities are built through informed governance, trusted relationships, and sustained collaboration. When elected officials understand the scope and value of public health, and when public health leaders understand the priorities, constraints, and opportunities facing policymakers, communities thrive. They are better positioned to prevent crises, respond effectively when challenges arise, and invest wisely for the future.
The contents of this toolkit can support elected and public health officials in convening broader coalitions, including business leaders, educators, healthcare systems, community-based organizations, and community residents. Cross-sector partnerships that reflect the complexity of today’s health challenges are key to addressing them.
The National Commission on Local Public Health Leadership calls upon local leaders to strengthen their relationships and reimagine what is possible when public health and policy leadership move forward together intentionally, transparently, and with a shared commitment to community well-being.
Appendix: Examples of Bulk Purchasing and Stockpiling Efforts
The National Commission also provides examples of existing mechanisms that promote a community’s ability to quickly draw from state- or federal-level resources or to leverage pre-existing relationships for bulk purchasing medication.
Because prescription drug costs and access have a substantial impact on state budgets and decision-making, one strategy attracting legislative attention is purchasing pharmaceuticals in bulk or joining a purchasing pool to increase negotiating power. By leveraging purchasing power across states or agencies, the goal is for all parties in the pool to receive lower prices.
Currently, five operational multi-state bulk purchasing pools negotiate deeper discounts on behalf of state and local agencies.
The National Medicaid Pooling Initiative (NMPI): Operational since 2003 and currently includes 10 states — Alaska, Kentucky, Michigan, Minnesota, Montana, New Hampshire, New York, North Carolina, Rhode Island and South Carolina — plus the District of Columbia. NMPI covers 3.8 million people and has supplemental rebate agreements with more than 90 pharmaceutical manufacturers.
The Top Dollar Program (TOP$): Starting with two member states in 2005, there are now six participating states: Connecticut, Idaho, Louisiana, Maryland, Nebraska and Wisconsin.
The Sovereign States Drug Consortium (SSDC): Founded as a non-profit structure in 2005, 13 states take part in the SSDC: Delaware, Iowa, Maine, Mississippi, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, Utah, Vermont, West Virginia and Wyoming. Collectively, the consortium covers 10 million people.
The Northwest Prescription Drug Consortium (NPDC): The NPDC is an intergovernmental agreement between Nevada, Oregon and Washington which provides broad pharmacy management services, operating under a single pharmacy benefit manager (PBM), which generates additional savings by aligning purchasing through one vehicle and leveraging those states purchasing power. Entities from both the private and public sector are eligible to join. Notably, the NPDC requires 100% pass-through of all manufacturer rebates and prohibits spread pricing.
Additionally, it provides a discount card program to residents in those states. Discounts are applied point-of-sale at participating locations. According to the consortium’s website, the NPDC facilitates more than $800 million in annual drug purchases for over 1 million people in participating groups and facilities. Since 2016, the program generated over $99.4 million in additional savings.
The Minnesota Multistate Contracting Alliance for Pharmacy (MMCAP): Founded in the mid-1990s, MMCAP is a group purchasing organization that combines the purchasing power of state agencies (such as public health departments), counties, cities and school districts in all 50 states to generate additional savings on pharmaceuticals and healthcare products. It does not include state Medicaid purchasing.
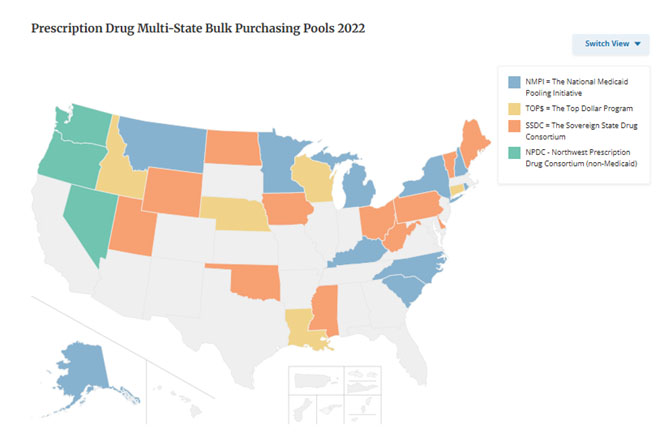
Image from The National Conference of State Legislatures. 2022.
Single-state Pools
Instead of pooling resources with other states, some lawmakers are consolidating the purchasing clout within their own borders. Created in 2019, New Mexico’s Interagency Pharmaceutical Purchasing Council is tasked with identifying strategies to leverage the collective purchasing power of the state’s agencies — including corrections, state employees and retirees, counties, public schools and universities — and report their findings annually to the legislature. Legislators use the information to inform fiscal policy in the state.
California embarked on a similar path in 2019 and, by executive order, required state agencies — including Medi-Cal, the state Medicaid agency covering 12 million people — to implement a combined drug procurement strategy. Implementation is in initial stages and, according to the California Legislative Analyst office, the potential savings generated could be hundreds of millions of dollars.
The Strategic National Stockpile (SNS) is a national supply of medicines and medical equipment that can be sent anywhere in the United States during a major emergency.
How the SNS Started
In 1998, Congress gave funding to the CDC to build a stockpile of medicines and vaccines to protect the public from biological or chemical threats and large disease outbreaks. The program was first called the National Pharmaceutical Stockpile (NPS).
In 2003, it became the Strategic National Stockpile (SNS) and was managed jointly by DHS and HHS. After the BioShield law was signed, oversight returned to HHS. In 2018, responsibility moved within HHS from the CDC to the Assistant Secretary for Preparedness and Response (ASPR).
The SNS is meant to support and resupply state and local public health agencies during national emergencies anywhere in the U.S. or its territories.
What is in the SNS?
The SNS contains large quantities of:
- Antibiotics
- Vaccines
- Antitoxins and chemical antidotes
- Antiviral drugs
- Life-support medications
- IV fluids and administration supplies
- Airway equipment
- Bandages
- Ventilators
- Other medical and surgical supplies
Some supplies are packaged as “12-Hour Push Packages,” which are ready to ship quickly. These make up less than 5% of the total inventory and include broad-use medicines and supplies for emergency care. The rest of the stockpile is managed inventory that can be tailored to a specific threat.
Who manages and requests the SNS?
HHS/ASPR is responsible for maintaining and delivering SNS supplies, and state and local health authorities are responsible for planning how they will receive, store, and distribute the supplies upon arrival.
State health departments, usually through their governor, can request SNS assets. National agencies like FEMA or the FBI may also request assets in certain situations. All requests are then reviewed by HHS/ASPR.
While these assets are available at the federal level, they may be difficult to access during times of emergency. Therefore, it is critical that local elected officials and public health officials understand where they can access supplies *locally* while waiting for federal assistance.
During the COVID-19 pandemic, when PPE was scarce, states created ways to supplement local stockpiles through policies and strategic partnerships.
The State of Iowa spent $45 million in purchase orders for masks, gowns, face shields, goggles, and other equipment from a variety of sources, including businesses that typically produce campaign signs and other promotional goods. Supplies were also brought in from the National Guard.
In Ohio, the governor engaged Ohio hospitals to compile and store PPE throughout the state. Establishing the stockpile was a joint effort between the Ohio Hospital Association, hospitals, and state agencies.
States also created regional supply chains to supplement federal aid during the pandemic. By consolidating multiple states’ PPE needs, they reduced costs and improved regional coordination of supplies.
- Bipartisan Policy Center. (December 2021). Public Health Forward: Modernizing the U.S. Public Health System. https://bipartisanpolicy.org/report/public-health-forward/.
- de Beaumont Foundation. (2025). Communicating About Public Health: A Toolkit for Public Health Professionals. https://debeaumont.org/resources/communicating-about-public-health-toolkit/.
- Cleveland Clinic. (2024, December 9). What Is Public Health? https://my.clevelandclinic.org/health/articles/public-health.
- National Association of County and City Health Officials. (2024). Local Health Departments Impact Our Lives Every Day. https://www.naccho.org/uploads/card-images/naccho-general/LHDs-Impact-Our-Lives-Every-Day.pdf
- National Association of County and City Health Officials. (2019). National Profile of Local Health Departments. https://www.naccho.org/uploads/downloadable-resources/Programs/Public-Health-Infrastructure/NACCHO_2019_Profile_final.pdf
- Blake, J. B. (1948). The Origins of Public Health in the United States. American Journal of Public Health and the Nation’s Health, 38(11), 1539–1550. https://doi.org/10.2105/ajph.38.11.1539
- Centers for Disease Control and Prevention. (1999, April 2). Ten Great Public Health Achievements — United States, 1900-1999. Centers for Disease Control and Prevention. https://www.cdc.gov/mmwr/preview/mmwrhtml/00056796.htm
- Centers for Disease Control and Prevention. (2011, May 20). Ten Great Public Health Achievements — United States, 2001–2010. Centers for Disease Control and Prevention. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6019a5.htm
- Starbuck, V., Lee, N., & Dean, C. (2025). Polarization in America: Survey of Local Government. CivicPulse. https://www.civicpulse.org/research/democracy-and-elections/polarization-in-america/may-2025.
- Levine, A. S. (2024). Collaborate Now! https://doi.org/10.1017/9781009411882.
- de Beaumont Foundation. (2025). Communicating About Public Health with Policymakers: A Toolkit for Public Health Professionals. https://debeaumont.org/resources/communicating-about-public-health-policymakers/
- de Beaumont Foundation and Harvard T.H. Chan School of Public Health. (2025). A View from 100 Days: Public Expectations About the Changing Public Health Landscape. https://hsph.harvard.edu/wp-content/uploads/2025/04/dBF-HSPH_100DaysPollReport_Apr-29-2025_final.pdf.
- Zink, A. (2026, April). Public Health Data Use and the Future of Public Health Data [Review of Public Health Data Use and the Future of Public Health Data].